
Language And Communication Disorders Of Autistic Children: An Interdisciplinary Approach

Abstract
Therapeutic approaches to prevention, intervention and speech correction in the case of children with disabilities but not only, especially of children with risk of developing autistic disorders may begin at birth. ASHA indicates the 24-30 months age interval as favoring language acquisition. The present study aims to analyze cases of children with various speaking and writing deficiencies, two of them having previously been diagnosed with autism. Several specialized interventions of an interdisciplinary team (psychologist, speech therapist, pre-primary school teacher) are also proposed. At school or in the family, by thoroughly analysing the process of oral language acquisition, one notes that almost all small children present dyslalia. The absence of therapeutic intervention in the cases of speaking disorders, both for typical children, but especially for autistic children, will lead in time, to their impossibility to develop socially and affectively and to the stagnation of the lifelong-learning process. The development of the educational system requires changes and action. The quality of education refers to identifying the dimensions of the didactic process, the learning contents, and the educational agents that may best support the education of all the categories of students, especially for children with language disorders and autism, ensuring their success in an open, flexible, efficient system.
Keywords: Autistic childrenlanguagepre-primary schoolcognitive development
Introduction
Specialized literature advances more theories on the communication mechanisms in the case of autistic children. The communication process entails
Problem Statement
At preschool age, the phonetic side of language prevails, although pronunciation is not yet perfect because of certain characteristics of the phonatory apparatus and of the verbal-motor and auditory analyser (Golu, Verza, & Zlate, 1993). Omissions are possible (in the case of joint consonants), replacements (e.g. place for lace, s for sh, l for r, etc.), sounds inversions (a change in the phonemes sequence). At the age of 6, the vocabulary reaches a maximum of 5.000, being preponderantly active.
By analyzing the indices of normal language development, one identifies several important stages in the evaluation of receptive and expressive language:
• age 3 – the child is able to render two stanza of a poem;
• age 4 – plural is employed in regular speech and in the use of pronouns (I, we, he, they);
• age 5 – the child uses verbs in the conditional mood and complex sentences. Mention should be made that, up to this age, the internal language has also developed. Internal language consists of auditory, visual, kinesthetic and motor components.
• age 6 – the child shows an interest in narrating events or actions that took place in the recent past or fictional histories. S/he describes the position or movement using prepositions: through, from, to, above, behind. The child is able to define some words. At the same time with language development, the stage of fixating the cognitive experience and that of activity organizing are also consolidated through psychomotor and motor structures. (Hategan, 2016).
The involvement of perceptive-motor structures in language development
- organization of corporeal scheme and laterality: identification of certain body parts and of their role; representation of the corporeal scheme and of its functionality; representation of actions; the body-environment relationship; the body-objects relationship;
- behavior and perceptive-motor structure of colour: colour identification, colour differentiation; operation- classification;
- behavior and perceptive-motor structure of form: identification, differentiation, operation;
- perceptive skills: kinaesthetic differentiation, spatial perception of positions, directions and size, visual differentiation: acuity, globular movement, constancy of perception, auditory differentiation, tactile differentiation;
- behavior and perceptive-motor structure of space: perception of space and one's rhythm and motion;
- behavior and perceptive-motor structure of space in the lexical or graphic fields, direction behavior in a spatial field: left, right, forwards-backwards, up-down; in space areas: near, far, very far;
- organization, spatial and temporal structuring: relating time to one, differentiation of chronological sequence, differentiation of duration of actions, events, etc.
Psycholinguistic profile of the autistic child
It is estimated that more than 50% of autistic people does not develop language, therefore cannot communicate on a regular basis, while some others can be, apparently, truly fluent in speaking. Autistic people who develop language usually start speaking later, in an unusual manner, specific to their disorder. Thus, verbal behavior is manifest through: immediate or retarded echolalia, pronoun inversion, rendering context without comprehension of the figurative meaning of some words or without understanding nuances and adapting communication to various social contexts, etc.
Research Questions
The aim of the research is that of identifying effective means in the process of recovering the preschool children’s language, including children with associated disorders, in our case, with autism. The study has started from several essential research questions:
How can one determine the language psychological age or the deficiency degree manifested by preschoolers at the communication level?
What difference does one note between dyslalic and non-dyslalic children after applying the test for acknowledging the language psychological age test?
What therapeutic methods can be applied in language research programs?
Is it necessary to introduce an educational model that includes alternative therapies in the preschool education?
In what follows, we intend to identify the language disorders observed in the preschool children subjects in the present research and to recommend several means of improving their language skills.
Purpose of the Study
Analysis of the results of the test for identifying the language psychological age
Preschool age is particularly important in language development. Lack of language communication leads to isolation, blockage at the level of social interaction, defective behavior. This study applies the test for identifying the language psychological age (Alice Descoeudres) on a group of 23 pre-schoolers, aged 4.5 - 6 (8 girls and 15 boys).
The test for identifying the language psychological age Alice Descoeudres (Vrasmas & Oprea, 2003)
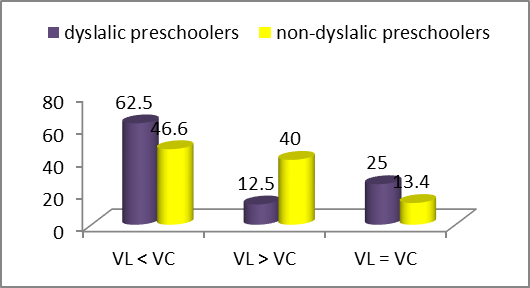
62.5% of the dyslalic children tested have a language psychological age lower than their biological age, in the case 25% of them, the ages correspond, and in only 12.5% cases, the language age is higher than the biological one. Language delays can be determined by inferior hereditary information or by social-emotional causes: family’s disinterest in the child’s language development or cerebral dysfunctions (autism). If the pre-primary school teacher elaborates individual files for psycho-pedagogical description of the pre-schooler and adopts differentiated teaching, it is possible for some dyslalic children to outgrow their biological age, from a linguistic perspective.
Research Methods
A pattern of therapeutic intervention. Team: psychologist, speech therapist, pre-primary school teacher.
Therapeutic program
General therapy was pursued with:
Physical exercises for the development of body mobility (neck, arms, hands gymnastics)
Exercises for the development of photo- articulatory organs (tongue, roof of the mouth, jaw bones – opening and closing the mouth, lifting the tongue to the roof, coiling the tongue towards the throat, swallowing, imitating coughing, stretching the lips with the mouth closed or showing teeth, imitating throat wash, gasping, panting, etc.)
Breathe learning was pursued as a game. Breathing therapy has two coordinates. It starts with breathing in the absence of speaking, which is a preliminary stage for breathing while speaking. Children were required to imitate various actions: blowing a candle, inflating a balloon, blowing in water with a straw, blowing the trumpet, pipe, whistle, flute, harmonica, paper sheets, steaming the mirror, move the paper boat on water, etc.
The use of myogymnastics with a musical background helped the children to relax during exercises.
The development of breathing while speaking was carried out by:
pronouncing vowels slowly, rhythmically, effortlessly during breathing-out;
rhythmic pronunciation of consonants or vowel groups (ai, ei, oi, ua, ue, etc.) while breathing out;
pronouncing syllables with vowel or vowel consonants groups while breathing-out (aie, oie, uie, sta, ste, stri, cra, cre, tre, tre, tre, etc.);
rhythmic breathing exercises accompanied by movement and singing (walking while counting, singing, reciting, telling riddles or proverbs that include the sounds which need to be consolidated).
The development of phonematic hearing was carried out using games such as:
The initial stage: identification of language disorders
According to the independent speaking test, in which the investigator (from the interdisciplinary team) pronounces sounds in order to have them identified in initial, medium and ending position), 8 children with logopathies have been identified, out of whom:
2 pre-schoolers, diagnosed with autistic disorders, omitted the sound r in certain words, and also sounds like ts, sh, z. These two also presented high attention deficit.
4 children substituted the sound sh with s. They were diagnosed with monomorphic dyslalia – parasigmatism.
1 child substituted the sound k with t. She was diagnosed with simple dyslalia.
1 child substituted the sound r with l and was diagnosed with monomorphic dyslalia – pararhotacism.
Among the dyslalic forms identified, parasigmatism is the most frequent pronunciation disorder (50%). According to the information in the literature, the sounds that are most affected are those occurring later in the ontogenetic development of the child: sounds r, s, z, sh and dj, these deficiencies being also obvious in the case of autistic children.
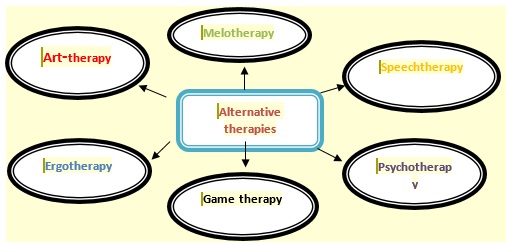
Alternative- applicative therapies
Correction in a timely manner of functional pronunciation deficiencies contributes in the decrease of reading/ writing mistakes, both at the pre-school and early school stage. To this end, we have employed various therapeutic programs for the correction of defective phonemes, applying alternative therapies useful in teaching children with language disorders and, particularly, children diagnosed with autism (figure
It has been acknowledged that game therapy has had a special impact on language stimulation and correction. Therapeutic game is the most effective means for language and thinking development of pre-schoolers. The game has multiple functions, making the autistic or dyslalic child open to communication more than any other alternative therapy.
Examples of game adapted to children with pronunciation disorders or associated disorders (in our case, autism): Lost Words – the game aims at enriching the active vocabulary of the child, at developing phonematic hearing, by the correct differentiation of sounds, at consolidating certain letters by realizing the phoneme-grapheme correspondence, and at developing attention in various contexts; Who Knows Wins! - the aim of this game is the correct observation and pronunciation of the sounds in a word, the differentiation of syllables, as well as the consolidation of the skill of correct writing of capital letters on the magnetic board, using 3D letters; the teaching game Change the letter/ change the syllable aims at developing thinking and language expressivity, phonological awareness (preschool children form new meaningful words by replacing the first or the last letter/ syllable), the main objective being the differentiation of the sounds in syllables, words and syntagma.
Findings
The analysis of the correction coefficient, obtained after using the test for phonological awareness (counting syllables, identifying consonants, naming the initial consonant, removing phonemes, etc.) shows that the lowest value was recorded for dyslalic children. However, after three week of individual and group therapy, dyslalic subjects, including the autistic ones, pronounced correctly a small amount of words, abiding by the phonetic laws (figure
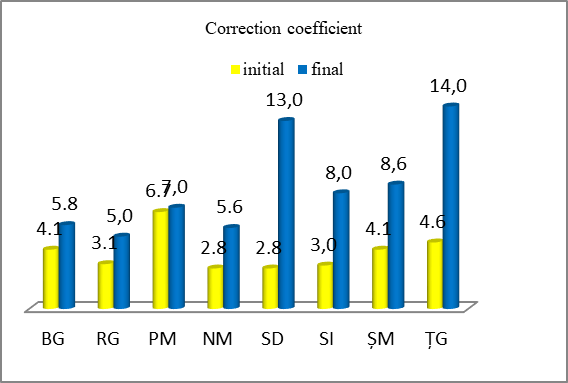
According to figure
After the therapeutic undertaking, 62.5% of the subjects with speech disorders have recorded progress in eliminating language deficiencies. The development of articulatory skills has especially focused on the materialization of reflected speech technique. The therapeutic program has combined varied therapies which make learning effective and help in the automation of defective phonemes. The language recovery process entails the elaboration of individualized programs applicable both in a specialized environment and at home. In the case of 37.5% of the subjects tested, lower progress has been recorded, owing especially to sound peculiarities, and to the passive involvement of the parents in the process of recovery.
Conclusion
Summarizing the aspects of educational therapy presented in this paper, one could conclude that the field of the recovery speech disorders is complex and in continuous transformation. Acknowledging and applying alternative therapies in speech therapy is a necessity at the preschool level. Educational programs should not only refer to autistic children or to children with defective pronunciation. Early prevention in what language acquisition is concerned is absolutely compulsory at preschool age. By educating speech at this early stage, the child’s adaptation and social integration is ensured, complex interpersonal relationships develop, and balance is achieved in the organization of psychic life. ]
References
- Baylon, Ch. (2000). Comunicarea [Communication].Iasi: Alexandru Ioan Cuza University Publishing House.
- Hategan, C. (2016). Logopedia [Speech therapy]. Bucuresti: Trei.
- Carroll, J. B. (1979). Psychometric approaches to the study of language abilities. In Fillmore, C.J., Kempler, D., & Wang. W-S.Y., (Eds.), Individual differences in language ability and language behavior (pp. 13-51). New York: Academic Press.
- Cungi, Ch. (1999). Cum să ne afirmăm [How to affirm ourselves]. Iași: Polirom.
- Golu, P., Zlate, M., & Verza, E. (1993). Child’s Psychology, Bucuresti: Didactic and Pedagogic Publishing House.
- Mureşan, C. (2004).Autismul infantil. Structuri psihopatologice şi terapie complexă [Childhood autism. Psychopathological structures and complex therapy].Cluj-Napoca: Cluj University Press.
- Vrasmas, E., & Oprea, V. (2003). Set de instrumente, probe şi teste pentru evaluarea educaţională a copiilor cu dizabilități [Set of tools, samples and tests for the educational assessment of children with disabilities].Bucuresti: UNICEF.
Copyright information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
About this article
Publication Date
15 August 2019
Article Doi
eBook ISBN
978-1-80296-066-2
Publisher
Future Academy
Volume
67
Print ISBN (optional)
-
Edition Number
1st Edition
Pages
1-2235
Subjects
Educational strategies,teacher education, educational policy, organization of education, management of education, teacher training
Cite this article as:
Barna*, I. (2019). Language And Communication Disorders Of Autistic Children: An Interdisciplinary Approach. In E. Soare, & C. Langa (Eds.), Education Facing Contemporary World Issues, vol 67. European Proceedings of Social and Behavioural Sciences (pp. 1638-1645). Future Academy. https://doi.org/10.15405/epsbs.2019.08.03.200